Care of an Artificial Eye and Related Information
Our artificial eyes are made of the finest quality of acrylic plastic (methyl methacrylate resin) which has been proven by use in dentures as well as in plastic eyes, beginning in 1939. We have made sure no irritating substances can be present in the finished prosthesis by the choice of materials and by our handling.
The shape of the eye has been fitted to the shape of the patients’ eye socket by our exacting MODIFIED IMPRESSION METHOD for your best possible comfort, eye movement and life-like appearance. It has been colored by a special method devised by us to match as accurately as possible the color and character of the companion eye and to give the appearance of living tissue.
GETTING USED TO THE PROSTHESIS
Most people become accustomed to the wearing of the artificial eye within a few hours and eventually many are not aware of its physical presence.
There are a few exceptions as, for instance, persons who completely lack tears to lubricate the under surface of their eyelids. From the beginning, such person will need some type of artificial lubricant, as will be discussed later in some detail.
INDIVIDUAL REACTIONS TO PROSTHETIC EYES
Each artificial eye wearer is an individual and can react differently from others. Some people who have been wearing artificial eyes for some time like to give advise to new wearers. They can only report what they have been told by someone else or what they have learned about their own individual cases.
Do not follow any advice offered by another eye wearer without consulting your ocularist or ophthalmologist or both, because such advice might be completely wrong for you.
Any special instructions your doctor or ocularist gives you personally should take precedence over any given here or by another patient.
HOW LONG SHOULD YOU WEAR THE EYE BEFORE REMOVING IT FOR CLEANING?
In our opinion you should discover by trial how long you can go. Wear the eye as long as it is not irritating and as long as it does not have material stuck to its front surface. After some experience you may be able to anticipate discomfort and clean the eye just before it would begin to cause trouble.
Many of our patients wear their eyes, without removal for cleaning, for one year between return visits for eye socket reevaluation and prosthesis polishing.
Only a few persons need to remove the prosthetic eye once each day for cleaning. Fewer yet remove and wash them morning and evening. Perhaps only one in many thousands find it necessary to leave the eye out during sleep, replacing it in the morning. Others wear their prosthesis for several weeks or a few months between removals for cleaning.
Scleral shell patients may require removal every night.
TO REMOVE THE PROSTHESIS FROM THE EYE SOCKET (see figure 1)
A. Wash and rinse hands thoroughly.
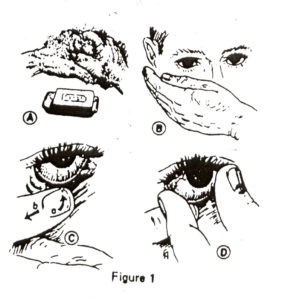
Figure 1
B. Face mirror (if this is over a lavatory, throw a towel over all hard surface – as illustrated in figure 2A). Tilt the head slightly downward while looking at the artificial eye in the mirror, this rotates the prosthesis into a favorable position for removal. Hold one hand, palm upward and heel against the mouth, below the eye socket to catch the prosthesis if it comes out suddenly.
C. Place the forefinger of the other hand against the middle of the lower lid, close to the eyelashes and parallel to them. Press the lower lid tissues backward until the lid margin goes under the lower edge of the artificial eye as in dictated by the arrow at (a). At the same time, pull the finger sidewise toward the cheekbone as indicated by the arrow at (b) to stretch the lid margin under the bottom edge of the prosthesis, exposing it to view. The effect will be like an edge of a button coming through a button hole.
D. If the artificial eye does not slide out of the socket by itself, the cupped hand may be taken away from the cheek and its forefinger and thumb used to grasp from under the upper lid. After removal, the eye should be rinsed or washed, being careful not to drop it down any drain.
CLEANING THE EYE
Never wash or dry the eye with any kind of cloth because it will slowly wear away the polished surface, creating a dull, non-lifelike appearance.
With the prosthesis already out of the socket, as described earlier, make your hands soapy with a mild hand soap such as Ivory or Palmolive and pick up the eye carefully because it will be slippery. Rub it vigorously with pressure from the tips of your soapy fingers. The water used can be as hot as the hands can stand- it could actually be hotter without harming the eye.
Rinse all soap from the eye and hands. Pat the surface of the eye dry with a soft facial tissue and check the surface to be sure there is not a thin film of material still stuck to it. If there is, the surface of the film will appear dull and you must repeat the cleaning process. If a film still remains, cleaning solution for hard or rigid gas permeable contact lenses can be used. Rinse under a good flow of warm water from a tap while rubbing the entire surface of the eye with the fingers to insure flushing away of any last remnants of material.
For further cleaning, soak in cleaning solution for contact lenses or return for polishing. Follow each name brand contact lenses cleaning solution instructions.
Put the rinsed prosthesis back in the eye socket wet.
TO REPLACE THE PROSTHESIS IN THE EYE SOCKET (see figure 12)
A. Wash hands. Face a mirror. If it is above a lavatory or other hard surface, drape a towel over that surface so that if the prosthesis is accidentally dropped, it is not likely to be damaged.

Figure 2
B. Hold the artificial eye by one hand in such a manner that the upper edge of the eye is upward and the back of the eye is toward the empty socket. One way to hold it is between the thumb and the second finger with the forefinger against the front of the cornea (over the pupil) as illustrated.
C. Lift the upper lid with a finger or the thumb of the free hand and keep the socket widely exposed for the next stop.
D. While watching in the mirror, slide the upper edge of the prosthesis up under the upper lid. Gradually, work it higher under the lid until most of the pupil and iris are hidden. Do not let it slide downward again until after the next step.
E. Release only the upper lid and bring the finger, which was holding it, around the front of the prosthesis to press it backward and keep it under the upper lid. Release the prosthesis from the grip of the finger and thumb of the other hand and bring the later down to roll the lower lid margin out from under the bottom edge of the eye.
F. When the lower lid is definitely out in front of the prosthesis, move it around until it seems that the artificial eye is seated in its proper place. Take both hands away from the eye slowly, being ready to catch the prosthesis if it has not been correctly placed and falls out. (Falling onto coarse, sharp or hard surfaces can ship or scratch the plastic eye.)
Sometimes difficulty in removing and placement of the artificial eye may be aided with the use of a suction cup. These can be obtained by contacting our office.
SOMETIMES EYE DROPS ARE NEEDED
The majority of persons do not need to use special eye drops on their artificial eyes when they have been carefully fitted by the modified impression method.
However, a small percentage of artificial eye wearers have fewer tears then necessary. Some have no tears from the major tear gland and practically no lubrication from the conjunctiva of the eyelids. In such cases there is considerable friction as the eyelids open and close, rubbing against the hard plastic surface. This can cause discomfort and enough disturbance of the eyelid tissues to give infections an easy start.
Those persons with dry eye sockets, whose eyelids close completely when they blink and when they sleep can use aqueous lubricating solutions such as artificial tears. There are several brands in the drug stores, which may be tried (Celluvisc). It is not possible to make specific recommendations because personal reactions to each varies so much. A lubricant which is very helpful to one person is often irritating or otherwise objectionable to other persons. Each eye wearer must discover for himself which lubricant is most helpful.
For dry eye sockets where the eyelids do not close during sleep, oily lubricants are needed because aqueous solutions evaporate and form hard, dry films across the front of the eyes which become irritating during blinking.
Some oils such as liquid petrolatum (mineral oil, Vasiline) tend to be irritating for most persons. Others such as tasteless castor oil and safflower oil are most often well tolerated and helpful. Another lubricant, medical grade silicone, has proven helpful to many persons, but it has certain characteristics which should be discussed with your ocularist before trying it. Others are Lacrilube, Refresh PM, and Artificial Eye Lubricant. Your ophthalmologist will need to prescribe other special drops for infections, allergies, etc.
As was said earlier many persons can wear properly fitted artificial eyes without discomfort or need for attention for the entire year between return visits for socket evaluation and polishing of the eye. Therefore, not everyone needs to be concerned that any or all of the following might be developed.
REASONS FOR DEVELOPMENT OF DISCOMFORT AND MUCOID DISCHARGE
A few socket which are perfectly comfortable in the beginning can become uncomfortable after a period of time. There are several conditions, any one or any combination of which can cause these changes. You should make a special point of remembering the following list of causes of discomfort and mucoid discharge for the remote possibility that one or more might develop, and remember the steps to be taken to correct them.
1. ROUGH-BUILD UP OF MUCOUS ON THE EYE
Some persons whose eyelids do not close completely over the artificial eye during sleep will have a partially dried film of ‘matter’ on the front of the eye when they wake in the morning.
Sometimes this can be cleared off without removing the eye by rubbing it with a rolled up tip of good quality facial tissue or q-tip moistened with warm water. Never use any kind of cloth for the reason already given, that it can dull the surface of the eye.
A few persons whose eyelids do close completely start as such a thin film that it can hardly be seen. This can make the surface of the eye just rough enough to irritate the underside of the eyelids as they blink. One should think of the possible presence of such a film if the eye socket is irritated with a scratching, burning or itching sensation.
The eye should be removed and carefully but thoroughly cleaned in such instances, in the manner described earlier.
2. FOREIGN BODIES UNDER THE EYELIDS
An eyelash can come loose or be broken off and be carried into the eye socket while replacing the eye. Dust or larger particles can blow into the eye socket. All can cause discomfort requiring removal and probably rinsing of the socket.
3. LOSS OF SURFACE POLISH OR DEEPER SCRATCHES ON THE PROSTHESIS
Dust in the air can get into the tear film and the scrubbing action of the eyelids during blinking can reduce the polish of the surface of the plastic. Accidental scratching of the front surface, even while the eyes are in the eye sockets, has happened for many persons. Dropping the eye onto hard, rough surfaces can cause irritation to the underside of the eyelids (scratches or chip in plastic).
The eyes must be re-polished to correct the problem. We recommend that the eyes be polished once each year to maintain comfort to the eye socket tissues and reduce any discharge, if present. If cracked or chipped, remove and call the Ocularist for repair.
Never try to smooth the plastic yourself as excessive material may be removed and cause a greater cost to repair. Many insurances now allow polishing every six months.
4. DISCOMFORT ACCOMPANING COMMON COLDS
With any common cold there may be some discomfort, mattering and discharge from the socket of the artificial eye while the companion, living eye does not seem to be affected.
Some persons have reported that removing the eyes and washing it once each day during the period of the cold and for a few days following helps to reduce the discomfort and discharge.
5. BACTERIAL AND VIRUS INFECTIONS
You must remember that the socket tissues around the artificial eye can become infected at least as easily as the companion, living eye. Discomfort and yellow-greenish discharge might indicate infection. Your tear duct (drainage) may be closed.
Your ophthalmologist must be consulted in such instances.
6. ALLERGIC REACTION TO VARIOUS SUBSTANCES
Many persons have mild allergies in the surface tissues of their living eyes without being aware of any discomfort. Allergies in the eye can be to such things as house dust, animal hair, plant pollens, milk, potatoes and other foods.
In our experience extending back 33 years, only one person has been allergic to a completely cured artificial eye which has been fabricated and cured pproperly. (On the other hand, incompletely cured plastic eyes and eyes made of ‘cold cure’ acrylic can very definitely cause trouble in the eye sockets). While we can not guarantee that one person in many hundred thousands will not be allergic to the perfectly fitted, fabricated and thoroughly cured plastic eye, we can assure you that the likelihood is extremely remote. Therefore, if allergy of some kind is suspected your ophthalmologist and possibly an allergist should be consulted.
7. EMPTY SPACE WHERE ‘STALE’ TEARS CAN COLLECT
The eye sockets of most person change in contour slowly over a long period of time. Probably due to effects of the eye removal surgery, fat atrophies from the depths of the orbit, reduction of contracted tissue, and possible implant migration. This increases the depth of the eye socket and pulls the back surface into new shapes which no longer fit the contours of the previously well fitted prosthesis. This causes pockets of space between the eye and the tissues. These can fill with tears which can lie there and become ‘stale.’ Apparently, salts precipitate out of the tears and irritate the tissues which, in turn, throw off muciod materials. In extreme cases, where the spaces are large, tears and mucous can spill out suddenly over the eyelid onto the face, sometimes an embarrassing occurrence.
The obvious correction for these problems is to refit the eye by taking a new impression on the back surface or, if the eye is too old, to fit an entirely new eye.
8. PROBABLY TOXIC SUBSTANCES WITHIN AN ‘OLD’ PLASTIC EYE; A DEVELOPMENT AFTER A LONG PERIOD OF TIME
Acrylic plastic (methyl methacrylate resin) has intermolecular spaces large enough for passage of water molecules. While the plastic eye is being bathed in the tear film, it takes up water very slowly. The water moves continually through the plastic carrying with it minute quantities of substances with small enough molecules to pass through spaces.
Very probably viruses and some bacteria can get into the eye prosthesis. Infection can go internal in the plastic, using antibiotics can eliminate infection in the socket but one may need to sterilize the prosthesis containing it. Very good evidence indicated that proteins collect in the plastic and that these cause irritation in the eye socket. For some persons, polishing or even refitting will not make such eyes comfortable.
The correction of this problem is simply to fit a new eye made of new plastic. We recommend replacement every 6-7 years; every 5 years for diabetics. Diabetics have a greater amount of acetone in their system which effect plastics and require replacement earlier.
STORING THE EYE
If the plastic eye must be left out of the eye socket overnight or longer for any reason, store it in water to which a bit of salt (1/4 teaspoon to a cup of water) has been added. They eye could be stored in any good contact lens soaking solution. If a plastic eye is allowed to dry out, the layers might separate at the painted surface. Keeping it wet prevents this. Another way to store the eye is in conditioning solution for hard or rigid gas permeable contact lenses.
POLISHING THE EYE
We recommend that the eye be polished at yearly intervals or as needed. This also affords the opportunity to check the eye socket and judge whether the back of the eye is still fitting the tissues of the socket properly.
Do not ever allow a dentist to re-polish the eye. Do not have any eye fitter except one we might recommend polish the eye. This is to guarantee that the shapes we have so carefully built into your eye for proper fit are not changed.
NEED FOR REFITTING THE EYE
Occasionally, not all the edema is gone from the orbit at the time of an original prosthetic fitting. As the edema disappears, which may take several months to a year, the artificial eye may sink deeper in the eye socket and the upper eyelid may droop over the eye. Whenever this becomes noticeable it would be best to add material to the eye beginning with a new impression taken on the back of the prosthesis.
As already noted earlier, slow atrophy of fat from deep in the orbit can require the same kind of refitting as above.
Occasionally, a person will have a sudden extreme loss or gain of body weight which will be accompanied by sinking back or other changes in the socket of the eye, requiring refitting of the prosthesis (commonly occurring during pregnancy).
WHEN TO CONSULT EITHER YOUR OPHTHALMOLOGIST OR YOUR OCULARIST
It is best to consult your eye doctor with any noticeable increase in tearing from the eye socket, with any marked loss or reduction of comfort, with excessive persistent mucoid discharge or with an easily recognized bulging out of the artificial eye. If there is an implant present, bulging could indicate extrusion or migration and should call for immediate attention. If your ophthalmologist feels a problems is one for the ocularist, he or she will suggest returning for a checkup on the prosthesis.
Sinking back of the eye so that the eyelids no longer open properly or a tilting into an abnormal direction of the prosthesis are reasons to see the ocularist.
The ocularist might be helpful in suggesting lubricants if they may be needed. Some problems require the cooperative efforts of both the doctor and the ocularist.
Call if you have any questions.
TO FURTHER HELP YOUR APPEARANCE
After we have made the ‘prosthetic side’ of your face match the ‘companion side’ by careful shaping of the eyelids and by lifelike coloring of the artificial eye, we will have recommended that you wear a pair of attractive protective glasses. These will distract from any asymmetries which we could not correct. Also, we many have prescribed Cosmetic Optics for the lens over the artificial eye, if desirable. This can cause further enhance lid shapes and contours. Polycarbonate lenses are recommended for their breakage resistance.
Beyond these aids, there are things you can do and others you can avoid doing to keep the artificial eye from being noticed.
1. Try to avoid body movements and head positions which will indicate to an observer that you are trying to hide something. Otherwise you most certainly will not hide it. Except for the following advice, just be as relaxed as you can – try to forget about having an artificial eye, and just be yourself.
2. Avoid tilting you head downward and at the same time looking up from under the eyebrows. Almost no artificial eye will move upward totally to match that of the companion ‘good eye.’ With your head tilted downward, your artificial eye could be looking at the floor while the companion is looking forward.
3. If your artificial eye will not move far to the sides, you should develop a firm habit of turning your head into the desired direction of gaze rather than just the eyes. Prosthetic eyes often move least in the lateral or temporal direction.
IMPORTANT POINTS TO REMEMBER AND WARNINGS
1. If the eye bothers so that it must be wiped or rubbed, always close the eyelids and wipe toward the nose. Wiping away from the nose can often cause the eye to fall out or rotate.
2. Never leave the eye in a piece of facial tissue. Several left in this way for just minutes have been picked up and thrown away. Some have been burned with the waste papers.
3. If you swim, dive or water ski, either wear a protective patch or swimming goggles – or remove the eye and store it safely. More eyes have been lost during these sports than in any other way.
4. Cold weather, dry weather and wind tend to make artificial eyes uncomfortable. Some lubricating eye drops may reduce or relieve this discomfort.
5. Never expose the artificial eye in any way to alcohol, ether, chloroform, some hair sprays, or any other solvents. These can damage the eyes beyond repair.
6. Be sure to remove the prosthesis before having any general anesthetic for surgery. Some of the anesthetics can damage the surface of the plastic, requiring expensive reprocessing or even replacement with a new eye. Others have been lost by the hospitals.
7. Always practice extreme cleanliness when handling your prosthetic eye. If your eye should happen to fall out, be sure to rinse it thoroughly and then wash it with soap and water before reinserting it.
8. Consult your doctor immediately if trouble you do not understand arises.
9. Have your eye checked and polished once a year to keep it in the very best condition. Do not let anyone other than ourselves, or someone we recommend, polish your eye. Polishing compounds used by many eye fitters, dentists, opticians and others will not polish as highly as necessary for greatest comfort. Also, the technician must take care not to change the contours of the eye, which might result in poor fit. Few understand the importance of the shapes which are achieved in the modified impression method we use.
10. Wear your protective glasses from the minute you have finished washing your face in the morning until you go to bed at night. Even when you are alone and least expecting it, an object can fly at your remaining eye. YOU NO LONGER HAVE A SPARE EYE. Protect the one you have.
11. Have your ophthalmologist check your good eye at least once each year.
12. As long as you are perfectly comfortable and the eye still looks fine, do not do anything between yearly check and polishings. Except for slowly changing appearance which you might not be aware of, if your eye needs care, it will let you know.
13. Never put the artificial eye in your mouth because it can cause choking and may lead to death.